Oxygen-enhanced MRI and multiple breath washout with Short extension reveal cystic fibrosis lung disease progression despite triple modulator therapy
RespiratoryOE
OE-MRI
Oxygen-enhanced MRI (OE-MRI) is a non-invasive functional imaging method that uses oxygen as the imaging agent to probe lung function and tumour oxygenation on standard clinical MRI systems.
Introduction
Oxygen-enhanced MRI (OE-MRI) probes tissue oxygenation by measuring MR signal changes that occur when a subject breathes increased concentrations of oxygen, typically moving from 21% to 100% oxygen for short periods of time.
Because oxygen is paramagnetic, its presence alters MRI relaxation properties and influences image contrast. Increased dissolved oxygen shortens T1, which forms the basis of most OE-MRI approaches. In the lung, elevated inhaled oxygen can also produce T2*-related signal changes because paramagnetic oxygen is present in the airspaces.
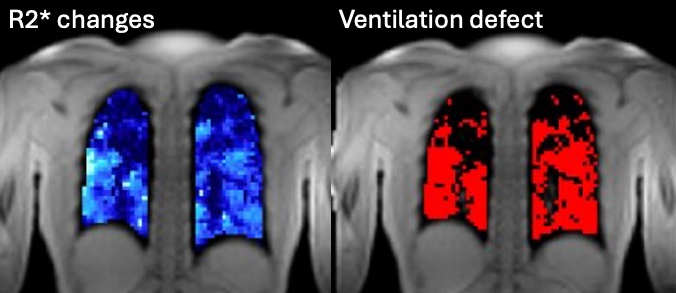
In the lung, OE-MRI is primarily used to assess regional ventilation and oxygen transfer. When different concentrations of oxygen are inhaled, signal changes can be detected in ventilated regions of the lung, providing a map of how effectively oxygen reaches different areas of the pulmonary parenchyma.
Depending on the MR sequence used, both T1 and T2* changes may be observed. These responses can be quantified in several ways, including relative signal enhancement or direct quantification of changes in T1 or T2*. From these measures, metrics such as ventilation defect percentage can be derived, indicating the extent of lung tissue that is not effectively ventilated.
OE-MRI reveals spatial heterogeneity in ventilation and oxygen delivery that structural imaging alone does not show. This is particularly relevant in diseases where regional lung function is locally impaired rather than uniformly reduced, including chronic obstructive pulmonary disease, asthma, cystic fibrosis, and other respiratory conditions.
A major strength of lung OE-MRI is that it provides functional information without ionising radiation and without injected contrast agent. This makes it well suited to repeat imaging studies, paediatric populations, therapy assessment, and research applications where safe and non-invasive measurement of regional lung function is a priority.
In oncology, OE-MRI is used to probe tumour oxygenation and hypoxia. Oxygen status is a critical feature of the tumour microenvironment because it influences tumour biology, aggressiveness, and response to treatment. By measuring how tumour signal changes during an oxygen challenge, OE-MRI provides insight into the extent and spatial distribution of oxygen-responsive tissue.
These measurements are based on oxygen-induced T1 changes, allowing OE-MRI to act as a biomarker of functional tumour oxygenation.
OE-MRI can also be combined with DCE-MRI to provide complementary information. OE-MRI reflects oxygen-responsive tissue, while DCE-MRI characterises tumour perfusion, vascular delivery, and microvascular function. Together, these methods support voxel-wise classification of tumour tissue as perfused oxygen-enhancing, perfused oxygen-resistant, or non-perfused.
Other Uses
Beyond lung and cancer imaging, OE-MRI has also been explored in organs and disease settings where oxygen function is physiologically important. In the kidney, OE-MRI may help probe regional oxygenation differences between cortex and medulla that are relevant to both acute and chronic renal disease.
Placental applications have also been explored, where oxygen handling is closely linked to placental function and dysfunction. These examples illustrate the broader potential of OE-MRI wherever oxygen delivery, uptake, or response is central to the biology being studied.
In Practice
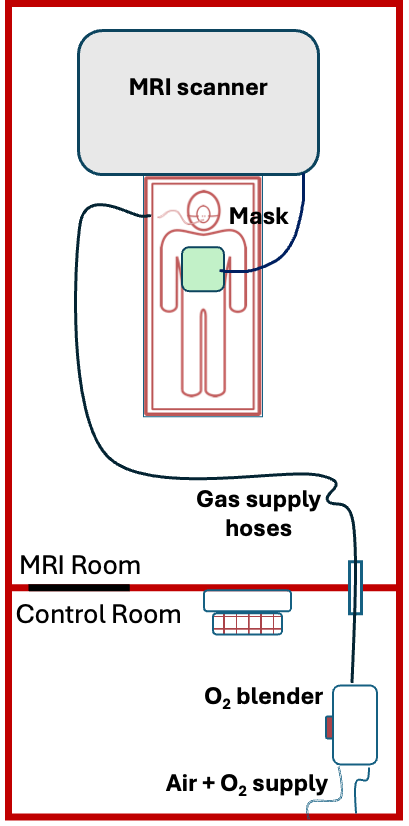
OE-MRI is a safe and well-tolerated procedure that can be performed on a standard clinical MRI scanner using standard coils and imaging sequences, making it a practical option for functional imaging studies.
The main additional requirement is a gas-delivery setup using masks alongside gas mixers placed in the scanner control room. These elements can be incorporated into the imaging workflow in a straightforward manner, helping to ensure subject comfort, protocol consistency, and reliable study execution, including in paediatric populations.
An OE-MRI experiment typically lasts 10 to 15 minutes and can readily be combined with additional imaging such as DCE-MRI or lung structural imaging.